Multidisciplinary teams
The multidisciplinary team (MDT)
Treating patients and improving their quality of life is the aim for all HCPs across therapy areas. Knowing the benefits of biosimilar therapy and recognising their potential in improving/optimising therapies will support this aim and help them in addressing the needs of their patients. Because of this, the MDT is a crucial element in the treatment process, with each member of the disciplinary team bringing unique skills in providing patient support. Hence, it is vital that the MDT receive full training around biologics, their impact on treatment, and has access to any supporting guidance to help with any challenges they may encounter.
Unmet need and limited access
Current guidelines often reserve biologics for patients with more severe disease and/or patients who have failed to respond to multiple other treatments.1 In some countries, access to biologics may then be further limited by the implementation of national eligibility and reimbursement criteria,1 creating an unmet need in many countries worldwide.
References:
- Edwards CJ, Hercogová J, et al. Switching to biosimilars: current perspectives in immune-mediated inflammatory diseases. Expert Opinion on Biological Therapy 2019; 19(10):1001-1014
Switch
Why switch from a reference biologic to a biosimilar?
In the past two decades, the treatment of debilitating, progressive diseases including immune-mediated inflammatory diseases (IMIDs) has been transformed by the introduction of biological therapies.1 However, the clinical benefits of biologic therapy are offset by challenges related to affordability of and accessibility to biologic medicines.2 Development costs remain a critical issue in biologic therapy affordability. Reference biologic drug development ranges around $1-$2 billion.3 Biosimilars on the other hand are less expensive to develop, costing around $200 million.4 This discrepancy in development costs explains how biosimilars may be more affordable, driving improved accessibility for patients.
References:
- Edwards CJ, Hercogová J, et al. Switching to biosimilars: current perspectives in immune-mediated inflammatory diseases. Expert Opinion on Biological Therapy 2019; 19(10):1001-1014
- Dutta B, Huys I, et al. BioDrugs 2020; 34: 159–170
- Blackstone EA and Fuhr JP. The economics of biosimilars. Am Health Drug Benefits 2013;6(8):469-478
Switching to a biosimilar: the do’s and don’ts of patient communication
Do’s
- Speak to the patient before the switch
- Talk about health-economic benefits of a non-medical switch
- Find out where patients collect information*
- Discuss any concerns you† and the patient may have
- Proactively arrange for feedback post-switch
- Offer them a compromise 6 months before an alternative therapy is considered
- Encourage contact with successful switchers
Don’ts
- Don’t leave the patient alone with only written information
- Don’t scare the patient with exaggerated or overly excessive lists of all potential AEs
- Don’t blame Dr Internet
- Never use the term ‘nocebo’
- Don’t say ‘cheaper’ – biosimilars are less expensive
- Don’t talk about statistics
- Don’t take a patient’s agreement for granted
- Don’t push patients for an immediate decision
*More side effects are reported by patients who use the internet.
†Costs or pressure from health insurance or representatives.
AE, adverse event.
Reference:
Adapted by Taylor P, Braun J, et al. Anti-TNF in rheumatic diseases: Inventory and outlook. EMJ Rheumatol 2018;5:36–43
For more on information on the MDT’s role in switching patients to biosimilars, please click on the following videos:
Can we live up to patient expectations?
19/11/2021 | 52:37
The crucial role of nurses in optimizing patient communication
19/11/2021 | 52:37

The importance of IBD nurses in discussing biologic switch with patients
19/11/2021 | 52:37

Improving patient communication through the understanding of their need to share the information
19/11/2021 | 52:37
Optimising communication through establishing trust with the patient
19/11/2021 | 52:37

To hear Associate Professor Fraser Cummings discuss real-world experiences with biosimilar switches, please click on the following video:
Satellite Symposium at ECCO Congress 2020
19/11/2021 | 52:37

Nocebo
Numerous studies have revealed non-adherence to prescribed therapies in a large proportion of patients with IMIDs including psoriasis, rheumatoid arthritis, Crohn’s disease, ulcerative colitis.1
A number of factors have been associated with non-adherence, including ‘non-specific side effects’, which have been attributed to the so-called nocebo phenomena2
References:
- Mitchetti P, Weinman J, et al. Adv Ther 2017; 34(1): 91–108.
- Barsky AJ, Saintfort R, et al. JAMA 2002;287:622–7
The nocebo phenomena: The negative equivalent of placebo
Placebo versus nocebo


- Nocebo effect: the induction or the worsening of symptoms induced by sham or active therapies1,2
- Nocebo response: new and worsening symptoms that are caused only by negative expectations on the part of the patient and/or negative verbal and non-verbal communications on the part of the treating person, without any (sham) treatment1
References:
- Häuser W, Hansen E, et al. Dtsch Arztebl Int 2012;109:459–65;
- Planès S, Villier C, et al. Pharmacol Res Perspect 2016;4:e00208.
Nocebo effects are a result of complex interactions between the patient, their surrounding general psychosocial situation, the healthcare provider, and the way information is delivered and received1,2
References:
- Planès S, Villier C, et al. Pharmacol Res Perspect 2016;4:e00208;
- Colloca L, and Miller FG. Psychosom Med 2011;73:598–603
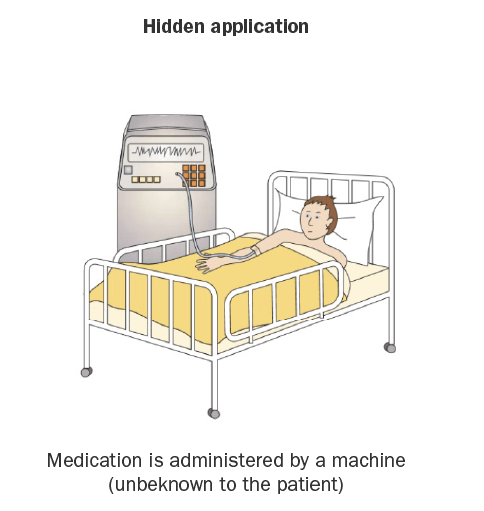
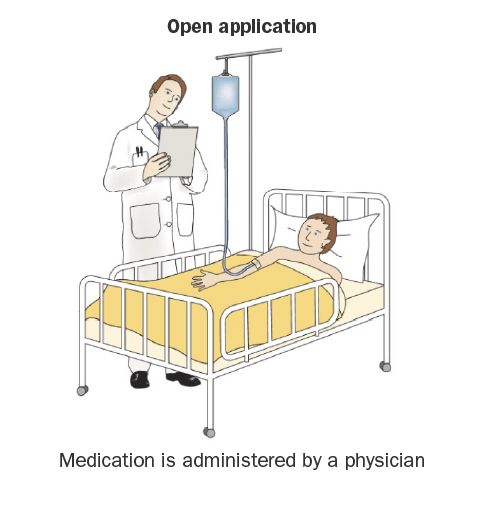
Placebo and nocebo effects are influenced by verbal and non-verbal communications
Negative expectations of the patient and/or negative verbal and non-verbal communications of the physician can contribute to a nocebo effect1,2


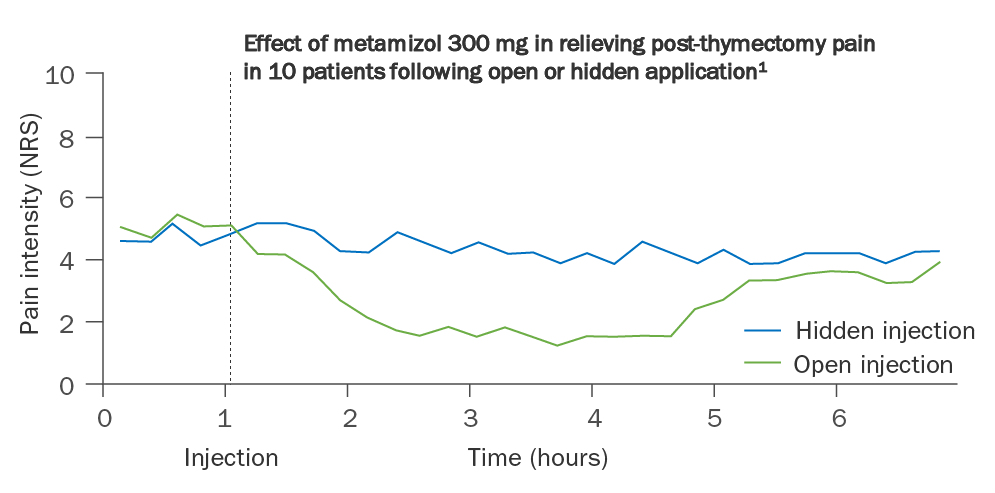
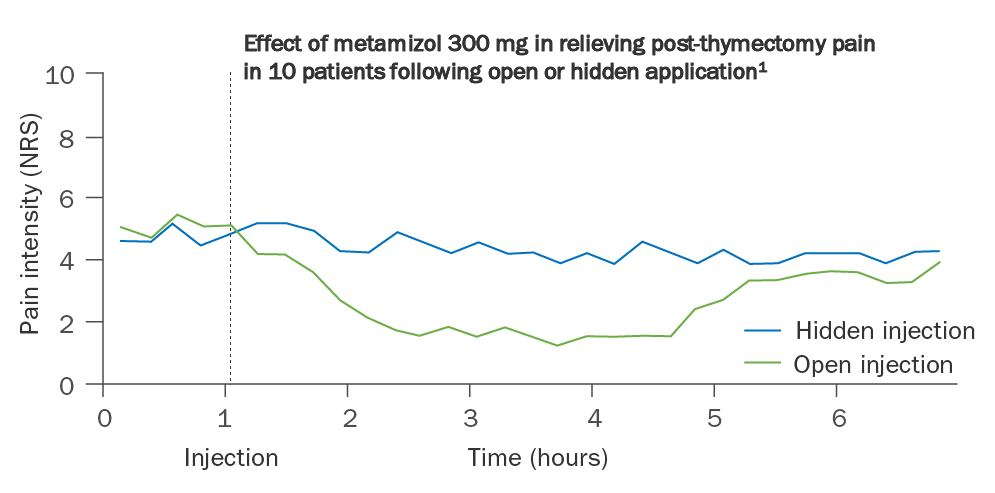
Adapted from Colloca L, Benedetti F. Nat Rev Neurosci 2005;6:545–52
References:
- Colloca L and Benedetti F. Nat Rev Neurosci 2005;6:545–52;
- Enck P, Bingel U, et al. Nat Rev Drug Discov 2013;12:191–204
Misattribution effects are closely related to nocebo effects
- Patients may misattribute pre-existing or unrelated symptoms to the effects of a drug1,2
- Somatic symptoms caused by pre-existing illness or anxiety and depression can be linked to negative expectations1
- The more symptoms that a patient has at baseline increases the risk that at least one of these symptoms will be misattributed to the treatment3
- Patients with expectations of developing side-effects are more likely to attribute symptoms to the treatment3
References:
- Planès S, Villier C, et al. Pharmacol Res Perspect 2016;4:e00208
- Faasse K and Petrie KJ. Postgrad Med J 2013;89:540–6
- Webster RK, Weinman J, et al. Br J Health Psychol 2018;23:436–54
Recently, discontinuation rates reported in clinical trials for patients switching from originator biologics to biosimilar drugs have been attributed to a possible nocebo effect1-5
References:
- Nikiphorou E, Kautiainen H, et al. Expert Opin Biol Ther 2015;15:1677–83;
- Glintborg B, Sørensen IJ, et al. Ann Rheum Dis 2017;76:1426–31;
- Tweehuysen L, Huiskes VJB, et al. Arthritis Rheumatol 2018;70:60–68;
- Glintborg B, Loft AG, et al. Ann Rheum Dis 2017;76:553–4;
- Scherlinger M, Germain V, et al. Joint Bone Spine 2018;85:561–7
Far-reaching consequences of the nocebo effect
Nocebo effect has been shown to impact the number of AEs experienced by a patient, resulting in perceived loss of efficacy, and leading to non-adherence1
Not only does this affect patients’ QoL, but it can also affect:1
- How HCPs resolve these additional AEs, which can lead to more complicated treatment regimens
- Needless switching of the patient to previous treatments
- Possibly reducing their future treatment options
Collectively, dealing with nocebo effects results in: 2,3
- Additional patient clinic visits
- More pressure on a healthcare system
- The cost savings of biosimilars not being realized
References:
- Rezk MF and Pieper B. Rheumatol Ther 2017. https://doi.org/10.1007/s40744-017-0085-z;
- Barsky AJ, Saintfort R, et al. JAMA 2002;287:622–7;
- Colloca L and Finniss D. JAMA 2012;307:567–8
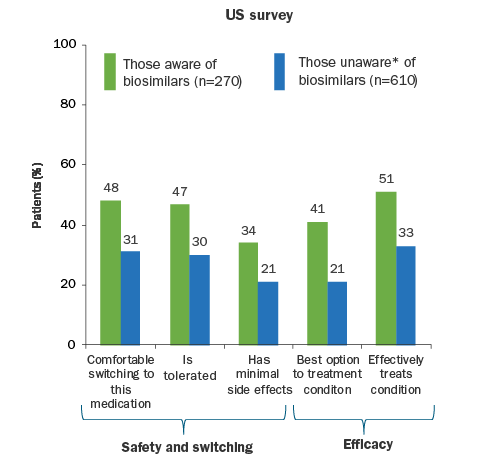
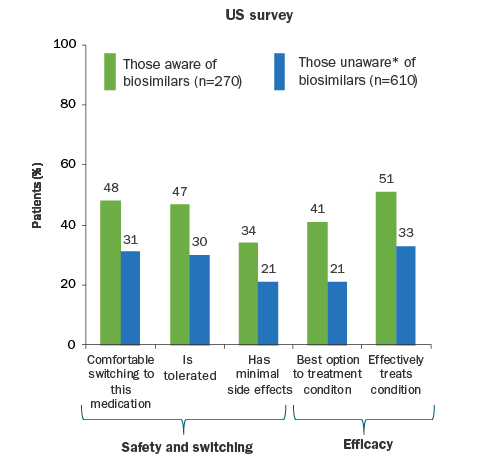
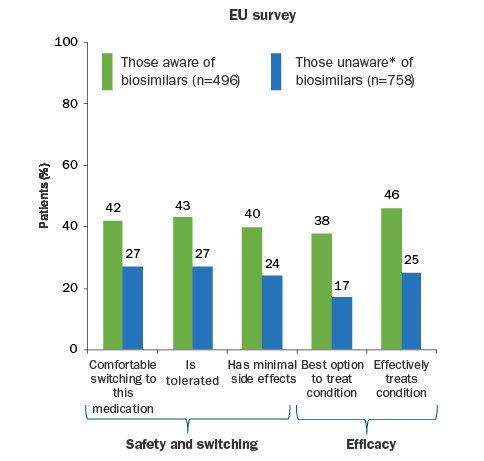
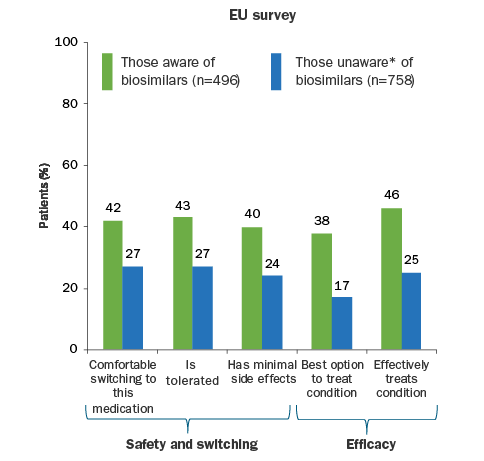
A lack of awareness of biosimilars amongst patients could be driving a nocebo response
Results of an international survey on biosimilars
Reference:
Adapted from Jacobs I, Singh E, et al. Patient Prefer Adherence 2016;26:937–48.
*Indicates the respondent answered 'never heard of a biosimilar' in response to the survey question "Which of the following types of medications have you heard of before today?"
The nocebo effect can be mitigated through physician and patient education, effective communication, and managed care programmes1-4
References:
- Zschocke I, Orland C, et al. J Eur Acad Dermatol Venereol 2017;31:1014–20;
- Colloca L and Barsky AJ. N Engl J Med 2020;382:554–61;
- Kristensen LE, Alten R, et al. BioDrugs 2018;32:397–404;
- Razanskaite V, Bettey M, et al. J Crohn’s Colitis 2017;11:690–6
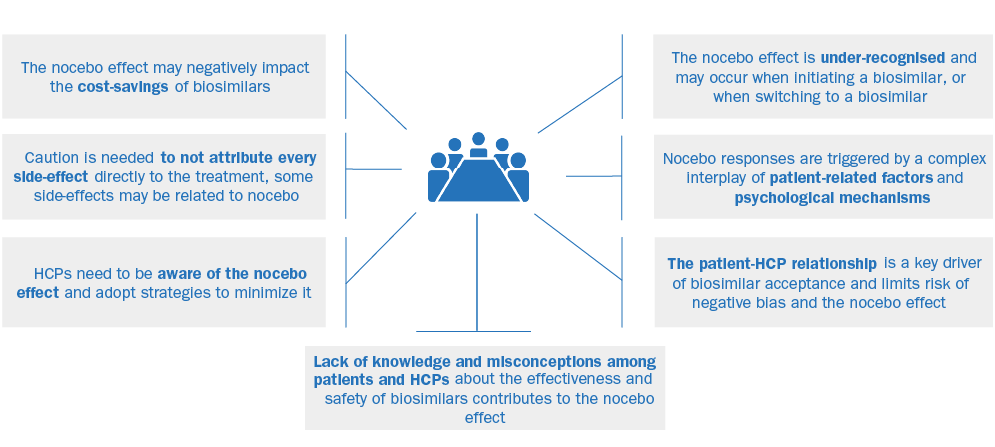
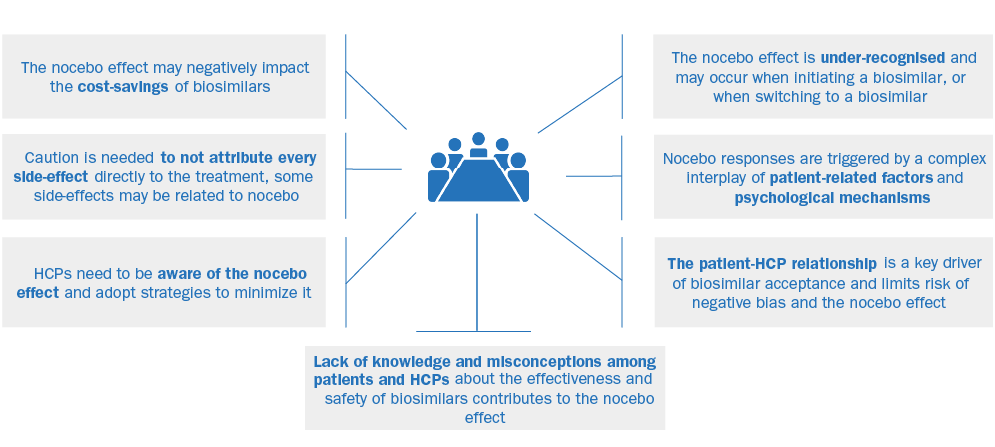
HCP awareness and understanding is key to minimize nocebo effects in patients treated with biosimilars
Reference:
Adapted from Pouillon L, Danese S, et al. Consensus report: clinical recommendations for the prevention and management of the nocebo effect in biosimilar-treated IBD patients. Aliment Pharmacol Ther 2019;49:1181–7